Microbial Risk Assessment
Probing Depth & BOP do not predict future loss of attachment. * The Diagnosis of Periodontal Disease in Private Practice.
Private Practice. Apsey et al J. Periodontol 2006;77*
¹Fluoride: Justified Concern
Because, unlike PD and BOP, the presence of pathological microbes predicts future loss of attachment. The problem with relying on PD is that it’s a lagging indicator. It can’t even be measured until the periodontal infection has already destroyed bone and attachment. As for BOP, it measures capillary fragility, not disease¹. There are many other things (probing force, hypertension, aspirin use, beta-blockers, oral contraceptives, etc.) that also cause gingival bleeding. So many that the probability of a false negative is 88%, i.e. 88% of non-bleeding sites are already infected².
In studies comparing traditional clinical diagnostic tests to microbial tests, none of the traditional clinical tests predicted future loss of attachment. Only the presence of specific species of pathogenic bacteria correlated with attachment changes on …individual teeth³. The question isn’t why bother with microbiological tests … it’s why are we still using 100 years old, inaccurate surrogates like notched metal sticks and blood when we should be looking for the specific pathogens that cause disease? Why aren’t we diagnosing infections with the same modern microbiological tests that physicians routinely use?
Periodontal infections are devious. Did you know, pathogens like Treponema denticola (1 of 57 species of
pathogenic oral spirochetes), Porphyromonas gingivalis, and Tannerela forsythia, don’t actually destroy tissue and
bone. Not directly anyway. When their numbers reach a certain threshold, they begin to secrete substances that upregulate over 60 genes in our T-cells including those that govern diapedesis, chemotaxis, and WBC proliferation, to initiate an aggressive immune response. Why you should be asking, would pathogens ever want to initiate an immune response? Because these sly invaders can also down-regulate 1,000 additional T-cell genes, especially those that inhibit phagocytosis. The end result: the influx of large numbers of impotent, short-lived WBC’s. When they die at the end of their 3-day lifespan, their unused enzymes destroy the local tissue, providing the pathogens with a rich source of nutrients. In other words, free lunch.
FDC Blue No. 1 Popular Misconception
 About half of the total pathogens in periodontal infections are spirochetes (Treponema). Their presence in subgingival biofilms is highly correlated with future loss of attachment (odds ratio=10.1, 95% CI, p=0.004). Phase microscopy easily detects all 57 species of oral Treponema. Large numbers of WBC’s, the hallmark of all periodontal infections, are also easily seen. In addition to detecting inflammatory WBC’s and all species of pathogenic spirochetes, there’s a tremendous additional benefit as well. Seeing one’s own ”squiggly bugs”, freshly taken from one’s mouth, on an ultra-high-resolution video monitor is, hands-down, the most effective patient motivator ever devised. When patients see the creepy-crawlies in their mouths, you don’t have to sell them on the benefits of therapy or being compliant with home care. They want those bugs out of their mouths … now, whatever it takes.
About half of the total pathogens in periodontal infections are spirochetes (Treponema). Their presence in subgingival biofilms is highly correlated with future loss of attachment (odds ratio=10.1, 95% CI, p=0.004). Phase microscopy easily detects all 57 species of oral Treponema. Large numbers of WBC’s, the hallmark of all periodontal infections, are also easily seen. In addition to detecting inflammatory WBC’s and all species of pathogenic spirochetes, there’s a tremendous additional benefit as well. Seeing one’s own ”squiggly bugs”, freshly taken from one’s mouth, on an ultra-high-resolution video monitor is, hands-down, the most effective patient motivator ever devised. When patients see the creepy-crawlies in their mouths, you don’t have to sell them on the benefits of therapy or being compliant with home care. They want those bugs out of their mouths … now, whatever it takes.
BANAZyme Enzymatic Assay
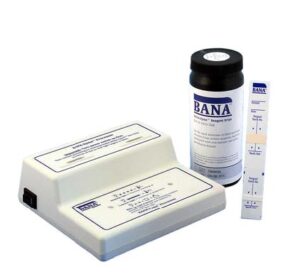 BANAZyme is a 5-minute, chairside enzymatic test for T. denticola, P. gingivalis, and T. forsythus. These are the most pathogenic species of periodontal pathogens and common to almost all infections. BANAZyme is as sensitive as DNA testing as documented in over 50 published studies. It’s easy too. Just place subgingival biofilm on the test strip and insert it into the fully automatic processor. See Processor
BANAZyme is a 5-minute, chairside enzymatic test for T. denticola, P. gingivalis, and T. forsythus. These are the most pathogenic species of periodontal pathogens and common to almost all infections. BANAZyme is as sensitive as DNA testing as documented in over 50 published studies. It’s easy too. Just place subgingival biofilm on the test strip and insert it into the fully automatic processor. See Processor
Didn’t find your answer?
¹NHANES, The Prevalence of Periodontitis in the US, J Dent Res 2012 91: 907-908
²Lang et al, J Clin Periodontol 17(10) 1990
³Bacteria Associated with Attachment Loss Renvert et al: J Periodontol 1996; 677:562-571